


We knew and greatly admired Dr. John Nagelhout, PhD, CRNA, FAAN, a CRNA whose life of teaching, research, clinical work, and program leadership eclipsed others of his generation. He was revered locally by his students and fellow colleagues and known widely as the principal architect of the book Nurse Anesthesia, the definitive treatise of our specialty. To the tens of thousands who have turned to his text seeking clarity or illumination, the book took on a kind of mythology of its own, referred to by most not by the formal rubric cataloged by the Library of Congress but simply as “Nagelhout.”
John recently passed. He was an elegant, soft-spoken, and humble man whose genius was evident in many ways. Today, we wish to revisit just one of his many accomplishments – our personal way of immortalizing and giving thanks to the man. We must start with the Taiwanese banded krait, a serpent nearly unrivaled for its hellacious venom. This krait’s neurotoxin kills many in its Southeast Asia and Northern China habitats. The primary active ingredient in that venom is α-bungarotoxin (α-Btx), a proteinaceous concoction that binds irreversibly to the nicotinic acetylcholine receptor (nAChr). Like a heat-seeking missile whose sole task is to bore down with savage intensity onto an enemy plane’s heat signature, α-Btx does the same with exquisite biochemical precision as it seeks out the nAChr, blocking the action of ACh. An agonizing paralysis, respiratory failure, and death await the envenomated victim in near-time. John knew this.
 The banded krait (Bungarus fasciatus)
The banded krait (Bungarus fasciatus)
John also knew that skeletal muscle saturated with α-Btx, irreversibly affixes itself to every Ach receptor on a one-to-one basis. Knowing the total amount of α-Btx that is exposed to the skeletal muscle (we will call that ‘α-Btx Total’), and armed with the knowledge that once attached to the nAChr, it stays put (we will call that ‘α-Btx Blocking’), then the amount of free α-Btx recovered (we will call that ‘α-Btx Recovered’) permits the precise quantification of the number of Ach receptors in the muscle sample. That is:
(α-Btx Total) – (α-Btx Blocking) = (α-Btx Recovered)
Now take that little equation a bit further:
(α-Btx Total) – (α-Btx Recovered) = (α-Btx Blocking)
Therefore,
(α-Btx Blocking) = quantification of the amount nAChr
The elegance of the pharmaco-biochemical rationale is foundational to a good deal of past, present, and likely future neuromuscular and neurophysiological research and clinical work. While we’ve simplified the complexities of its measurement, this gives us a good sense of how to determine the density of nAChr in skeletal muscle.
A life-saving observation
As entry-level students in the specialty, we all learned that the administration of succinylcholine to a burn patient (among a few other scenarios as well) could produce nearly instantaneous cardiac arrest due to profound hyperkalemia. Before John’s time, the mechanism was poorly understood, and several hypotheses were proposed, but the science had not kept up.
We contacted a close CRNA colleague and friend of John’s, Valdor Haglund, who worked with him on various clinical and research activities. He shared details about a patient John and other colleagues cared for. The unfortunate man experienced devastating 2nd and 3rd-degree burns over 80-90% of his body and was tended to in the institution’s burn unit for many procedures over a period of many months. John and colleagues designed a study to address their hypothesis, and with full consent, while the patient was under anesthesia for regular burn debridement and grafting procedures, skeletal muscle tissue samples were harvested and exposed to α-Btx. A remarkable observation was made, which lives in infamy and provides a mechanistic explanation that has prevented many deaths, warning us of the perils of using succinylcholine in burn-injured patients. An explanation directly traced back to John.
Here, published with permission, is the original graph from John’s momentous publication in the journal Anesthesiology decades ago. This graph clearly and quantitatively demonstrates the time course of the proliferation of extra-junctional nAChr in a burn patient.
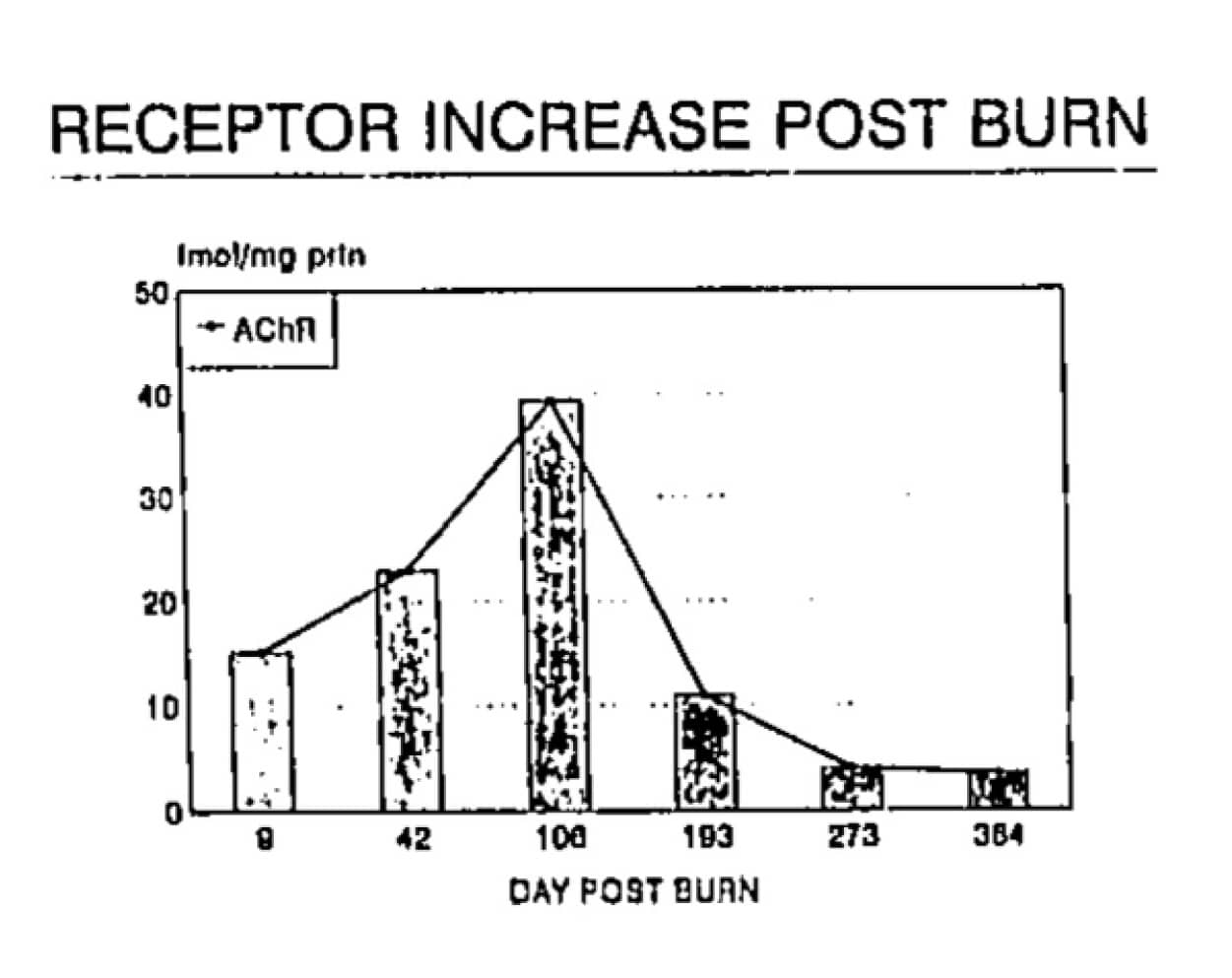
With kind permission. Anesthesiology. September, 1994;81:A1089.
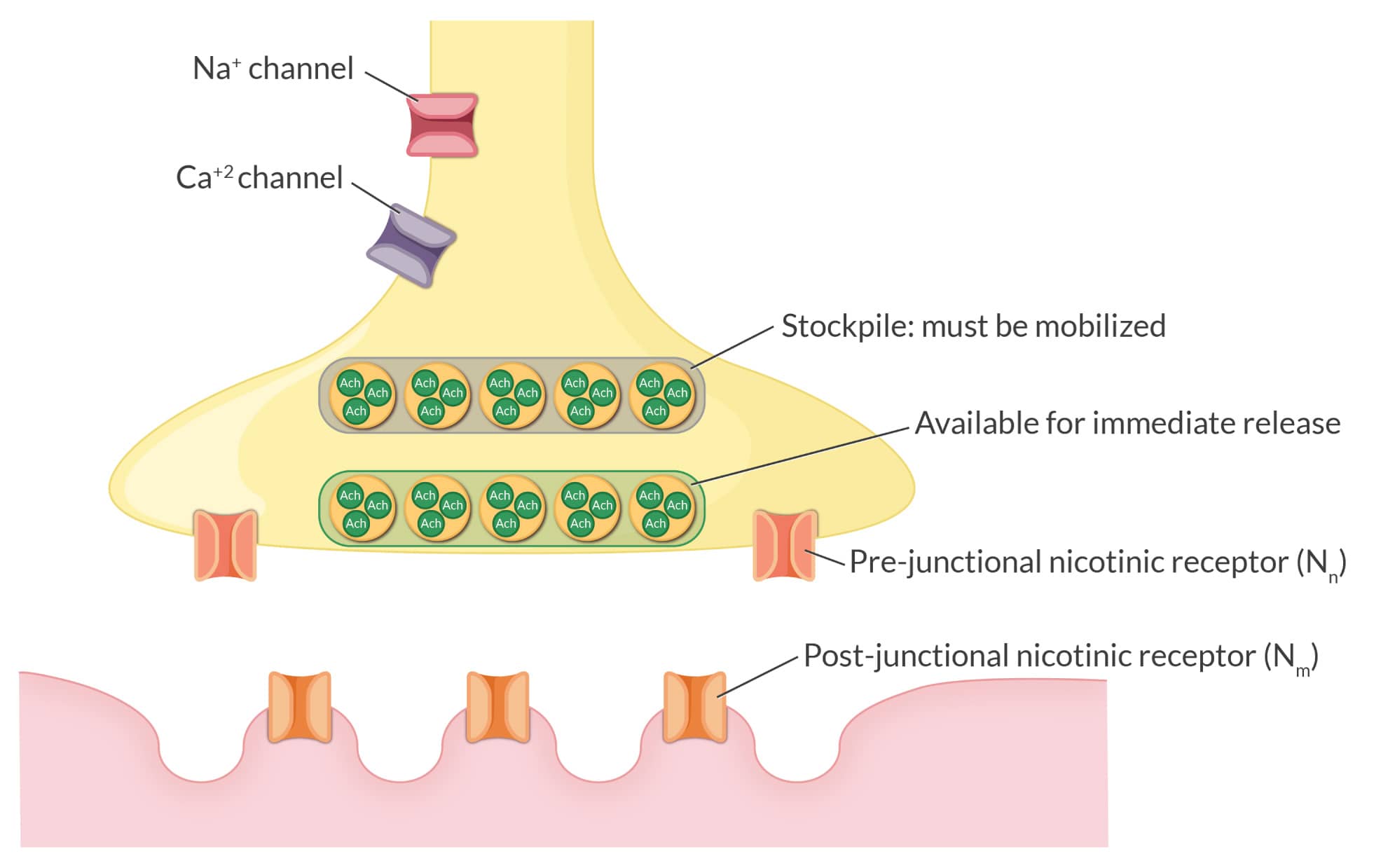
The nAChr in skeletal muscle is usually positioned strategically at the edges of the junctional folds at the neuromuscular junction on the postsynaptic side. Following ACh activation, Na+ and K+ diffusion results in depolarization, permitting muscular contraction in a graded manner. This gradation allows us to precisely quantify skeletal muscle activation, permitting us to lightly brush a baby’s cheek or heave a heavy load of dirt into a wheel barrel. Despite a high intracellular K+ concentration, what is usually liberated into the serum with succinylcholine administration is physiologically insignificant. However, with extrajunctional proliferation of nAChr, creating new “spigots” on the muscle cell membrane for K+ to emerge, serum K+ can rise dramatically and potentially catastrophically. We can look to John for illuminating the precise mechanism for why we must avoid succinylcholine in scenarios of extrajunctional spread of nAChr in burn injury and other scenarios like paralysis, immobilization, and certain myopathies. Thank you, John.
A life that inspired others
John may have been the first CRNA to obtain a PhD in a basic science, who then marshaled that knowledge and skill set to inform the evidence-based practice of anesthesiology using the tools of science guided by a keen intellect. His students and contemporaries lauded him as a polymath, and for good reason. To this day, few can put forth a comparably eclectic and accomplished curriculum vitae of professional and life experience.
Rest in peace, John Nagelhout. We are all grateful for what you accomplished and your legacy of teaching, research, clinical work, and program leadership, which continues to inspire many of us.
Related Articles


